An updated drug selection, stepwise prescribing, and a clear guide to what should—and should no longer—be on the prescription pad.Article published in MIMS DOCTOR Malaysia May 2026
BY Dr Sanjiv Rampal,Orthopaedic Consultant
I am pleased to share that my latest article, “Topical first, opioids never: Navigating the new pharmacological hierarchy in knee osteoarthritis,” has been featured in the May issue of MIMS DOCTOR Magazine Malaysia!
As general practitioners (GPs) serve as the crucial gatekeepers in primary care, aligning daily clinical practice with the latest global evidence is essential to improve long-term functional outcomes and safeguard patient safety.
This feature provides primary care physicians with a clear, practical, and updated drug selection framework backed by the AAOS 3rd Edition Clinical Practice Guideline (2021) and NICE NG226 (2022).
A summary of the core management updates detailed in the article is provided below.
🔍 Article Summary: Updating the Knee OA Prescribing Paradigm
1. The Non-Pharmacological Foundation
Before introducing medication, structured exercise and weight management remain the highest-priority, first-line interventions. Pharmacotherapy should always be viewed as an adjunct to—not a replacement for—these core lifestyle measures. Additionally, for patients managing obesity and diabetes, optimizing metabolic care (such as utilizing GLP-1 receptor agonists) can serve as an excellent “surgical adjunct” to reduce pain and boost overall patient satisfaction.
2. The New Stepwise Prescribing Hierarchy
Clinical guidelines have moved away from traditional defaults. Primary care providers are encouraged to adopt this evidence-based escalation pathway:
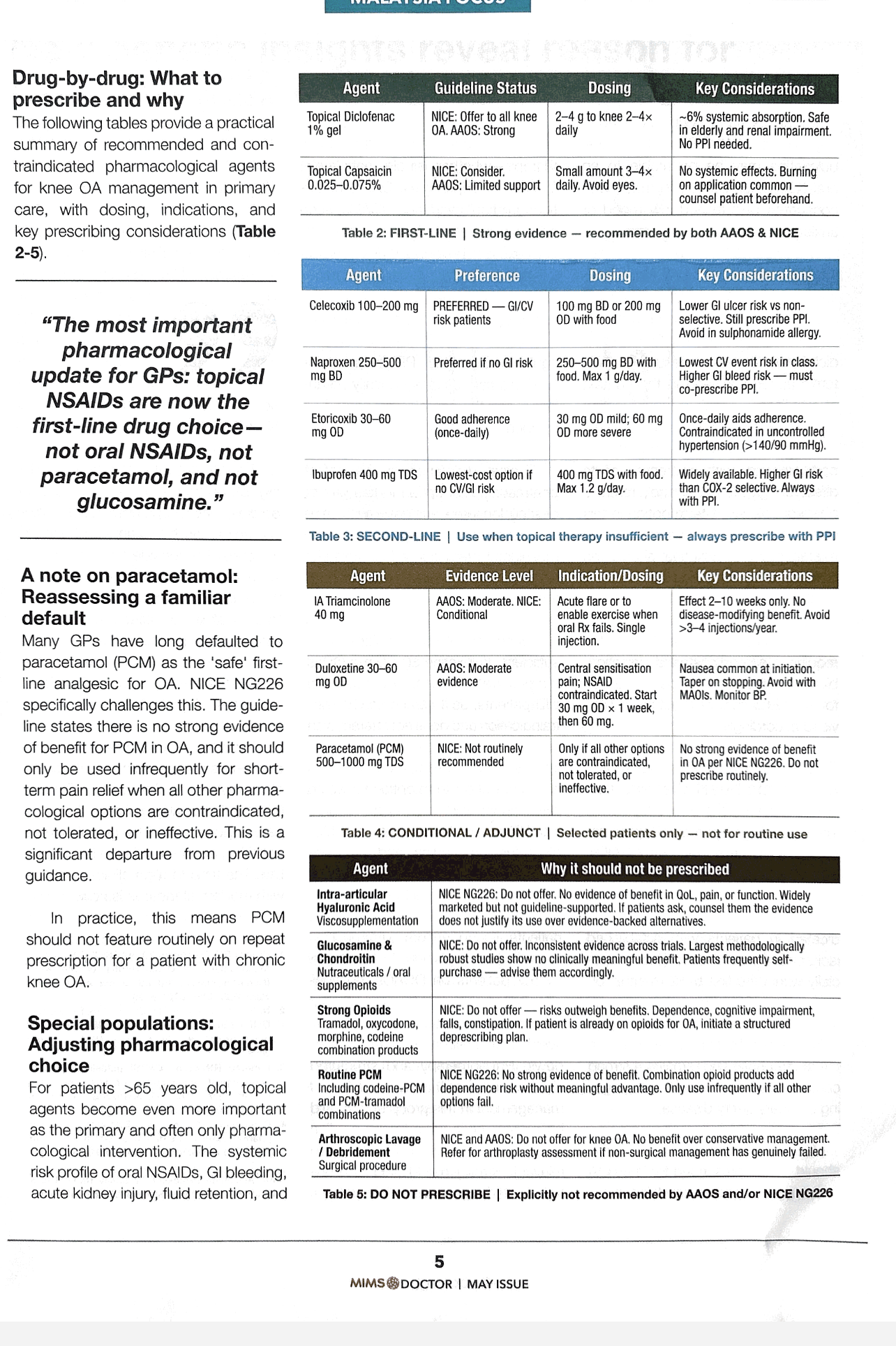
- Step 1: Topical NSAIDs (First Line)
- Protocol: Diclofenac 1% or 1.16% gel applied 2–4 times daily.
- Why: Offers comparable efficacy to oral NSAIDs with minimal systemic exposure, making it the safest choice for elderly patients or those with cardiovascular and gastrointestinal risks.
- Step 2: Oral NSAIDs (Second Line)
- Protocol: Use the lowest effective dose for the shortest duration.
- Crucial Practice Update: Always co-prescribe a Proton Pump Inhibitor (PPI) for gastroprotection, regardless of the patient’s age. Prefer Celecoxib for high GI-risk patients, and Naproxen for those with higher cardiovascular safety needs.
- Step 3: Intra-articular Corticosteroids (Conditional/Adjunct)
- Protocol: Reserved for acute pain flares or to help a patient engage in physical therapy. Relief is short-term (typically 2–10 weeks) and should not exceed 3–4 injections a year.
- Step 4: Duloxetine (Central Sensitization)
- Protocol: Consider when oral/topical NSAIDs are completely contraindicated, or if the patient experiences chronic musculoskeletal pain with concurrent anxiety/depression.
3. What to Stop Prescribing (The “Do Not Offer” List)
To protect patients from financial burdens and avoidable side effects, it is time to actively de-prescribe outdated treatments:
- ❌ Paracetamol (PCM): No longer recommended for routine, chronic use in knee OA due to a lack of strong evidence of benefit.
- ❌ Glucosamine & Chondroitin: Large, methodologically robust studies demonstrate no clinically meaningful benefit.
- ❌ Viscosupplementation (HA Injections): Explicitly advised against by NICE NG226 due to lack of quality-of-life improvements.
- ❌ Strong Opioids: The risks of dependence, cognitive impairment, and falls vastly outweigh the benefits. Active deprescribing plans should be initiated for patients currently taking them for OA.
Take-Home Message for Malaysian GPs: “Topical first, oral NSAIDs (with PPI) second, and opioids never.” Let us align our clinical habits with modern evidence-based standards to directly elevate the quality of life for our knee OA patients.
👉 Read the full guide and explore the detailed dosing tables for special populations (CKD and Ischemic Heart Disease) in the May Issue of MIMS DOCTOR Magazine.

#Orthopaedics #KneeOsteoarthritis #PrimaryCare #MedicalEducation #MIMSDoctor #EvidenceBasedMedicine #IMUUniversity

Leave a comment